
Orthognatic Surgery
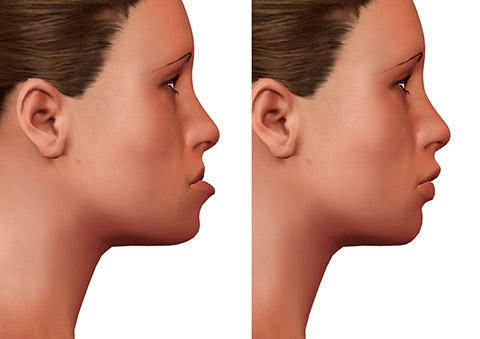
Orthognathic surgery; It is the name given to surgical interventions aimed at the treatment of problems such as biting, chewing, swallowing, speech disorder, breathing disorder, facial asymmetry and sleep apnea due to impaired lower and upper jaw relations. Defects in the skeletal structure as a result of congenital and developmental disorders of this region have disrupted the lower/upper jaw relation. Functional and anatomical corrections provided by surgical intervention bring beautiful changes in the facial profile and aesthetic appearance.
Jaw closing disorders may result from the relationship of the teeth to each other or the bones where the teeth are located. If the contact between the teeth is not as it should be, the bite is impaired and the treatment is done by the orthodontist. However, if the problem is in the bone roof, surgical treatment is required. After orthodontic treatment, the treatment is completed with orthognathic surgery. Skeletal jaw closing disorders are roughly called class 2 (closing where the lower jaw is behind) and class 3 (closing where the lower jaw is more forward). Normal closure is class 1 closure. There are other skeletal problems named according to malocclusion.
Orthognathic surgery is performed under general anesthesia. Le Fort 1 Osteotomy is performed for the upper jaw, Sagittal Split Ramus Osteotomy is performed for the lower jaw, and chin tip osteotomy (genioplasty) is performed for the chin tip. Surgery for each jaw takes approximately 2 hours. Since all incisions are made inside the mouth, there are no incision marks on the face. Unless there is abnormal bleeding, a blood transfusion is not needed. Especially in lower jaw surgery, the nerves and blood vessels of the lower jaw are carefully protected. Temporary or permanent numbness may develop in the lower lip if a cut or crush occurs due to squeezing, cutting or moving in an abnormal place. In cases of rupture, surgeons with microsurgery experience can easily handle it. Especially during upper jaw surgery, problems at the base of the nose and septum deviations can be solved simultaneously. Small touches can be made to the nose and lips. Septum deviation may develop as well. After the upper and lower jaw incisions, the jaws are placed in their new places with MRI-compatible titanium alloy plate and screws. The incisions inside the mouth are closed with dissolvable stitches. Edema develops on the face in the first 5 days after the surgery and gradually decreases. After approximately the third day, the lower upper jaw is connected to each other under the guidance of the plate, allowing it to heal in ideal closure. The average hospital stay of the patient is 2-3 days unless there is a special need. During this process, the patient is fed liquid food with the help of a straw. Oral care is very important during this period. Antibiotic treatment is administered for two weeks. Although it varies depending on the situation, the elastics are removed after 3-4 weeks and jaw movement is allowed. Feeding with soft food is started. After 3-4 months, the bones become largely safe and the edema decreases.
Who Can Have Orthognathic Surgery?
Orthognathic surgery can be performed at any age, but it is generally applied to people with skeletal deformities in the lower or upper jaw, especially after the age of 17-18, when development is completed. These deformities can generally be in the form of overgrowth, underdevelopment of the lower or upper jaw, or facial asymmetry. On the other hand, mandatory treatment of severe orthognathic problems as a part of some syndromic congenital anomalies requires experience and a multidisciplinary approach.
Is Orthodontic Treatment Necessary Before the Surgery?
The main goal in orthodontic treatment is to ensure the ideal closing relationship of the lower and upper jaw. This treatment is usually necessary before orthognathic surgery to ensure good alignment and leveling of the teeth and to correct the angles of the teeth. Braces are placed during or after preparation for orthodontic treatment. Orthodontic treatment usually starts after the age of 11-12. It is done after the permanent teeth emerge, in other words (ideally) between the ages of 12-18. Orthodontic treatment and its planning are very special and it is very important that this planning is done and carried out by orthodontists who know the preparation for surgery and are experienced in this regard. Poor planning and poor orthodontic treatment can lead to very serious problems. Surgical treatment of patients with malocclusion due to skeletal problems is sometimes ignored and attempts are made to correct it only with orthodontic treatment for the teeth. This leads to bad results. Since the underlying skeletal problems are not resolved, the teeth return to their previous positions, the teeth become mobile because the tooth roots are overstressed, the gums recede, and aesthetically inadequate results are obtained. In order to avoid these problems, it is important and necessary to have an experienced orthodontist in the treatment team and get an opinion from an experienced plastic surgeon to plan the treatment. The cost of correcting incorrectly started orthodontic treatment is high.
Orthodontic treatment is continued for a certain period of time to ensure ideal closure after surgical treatment.
Planning Jaw Surgery in Orthognathic Surgery
When orthodontic treatment is completed, cephalometric (side head radiograph) measurements are taken. Bite plates are prepared from the measurements taken from the teeth. If surgery will be performed on one jaw, 1 bite plate will be prepared, and if surgery will be performed on both jaws, 2 bite plates will be prepared.
These bite plates are used as guides during surgery to ensure the ideal position of the jaws relative to the skull base and the ideal tooth relationship – occlusion.
Evaluation of Structural Features of the Face in Orthognathic Surgery
When evaluating an orthognathic surgery patient, the height of the face is divided into approximately three parts. Upper face (forehead – skull base), midface (upper jaw – maxilla) and lower face (lower jaw). These three sections are approximately equal in height. The golden ratios on the face defined by Lenardo Da Vinci are a very important guide. These measurements to be made on the patient’s face give us a clinical idea about the proportions and balance of the face itself. On the other hand, the relations of these sections according to the anterior-posterior and right-left axis and the continuity of the midline, the location of the chin tip and the aesthetic appearance are combined with cephalometric data. The face is evaluated as a whole. Model surgery, digital virtual surgery and planning are combined with clinical findings to obtain the most ideal result. After these, the plan of the surgical intervention becomes clear. Facial anatomy varies according to race and also varies between individuals.